Arizona Child Fatality Review Program | Twenty-Eighth Annual Report
Firearm Deaths up 41%; Arizona’s Pediatric COVID19 Death Rate 250% Higher Than the National Average
Back in the mid 1990’s the AZ State Legislature established the Arizona Child Fatality Review Program to evaluate every child death and provide evidence-based policy recommendations to prevent child deaths.
Over the years many policy and operational interventions came out of these reports, from safe sleep to new seat belt laws for kids. The goal of each year’s report by conducting a comprehensive review of all child deaths and make policy recommendations to prevent as many as possible.
The Arizona Child Fatality Review Program published their 28th annual report last week. In 2020, 838 children died in Arizona, an increase from the 777 deaths in 2019. The leading causes of death were prematurity, congenital anomalies, motor vehicle crashes, poisonings, and firearm injuries. Prematurity was the most common cause of death for neonates (infants less than 28 days old) while suffocation was the common cause of death among infants 28 days to less than 1 year of age.
The accidental injury death rate increased 31% from 2019 to 2020. The top causes of accidental death were car crashes, poisonings, and suffocation. A child protective services history with the family, substance use, and poverty were the most common risk factors.
The firearm injury mortality rate increased 41% while car crash death rate increased 54%. The most common risk factor contributing to a firearm injury death was access to firearms. Eighty-six (86%) of firearm deaths involved a pistol (with the child’s parent often being the owner of the pistol).
Most of the Sudden Unexpected Infant Deaths (SUIDs) were due to unsafe sleep environments. Unsafe sleep environment was a factor in 100% of these deaths while objects in sleep environment was a factor in 92% of SUIDs.
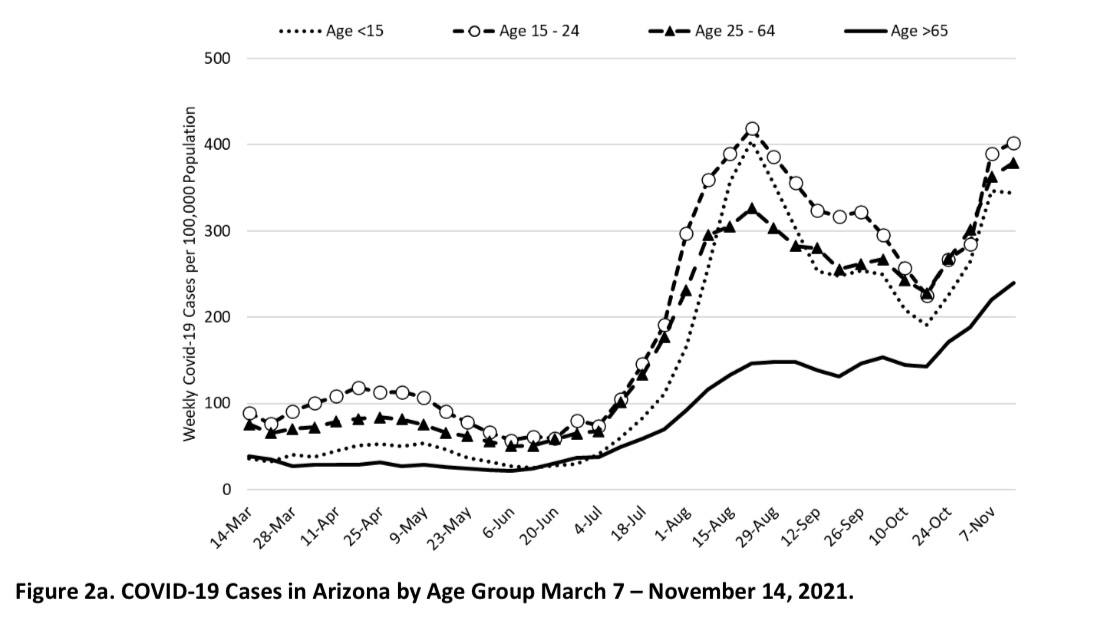
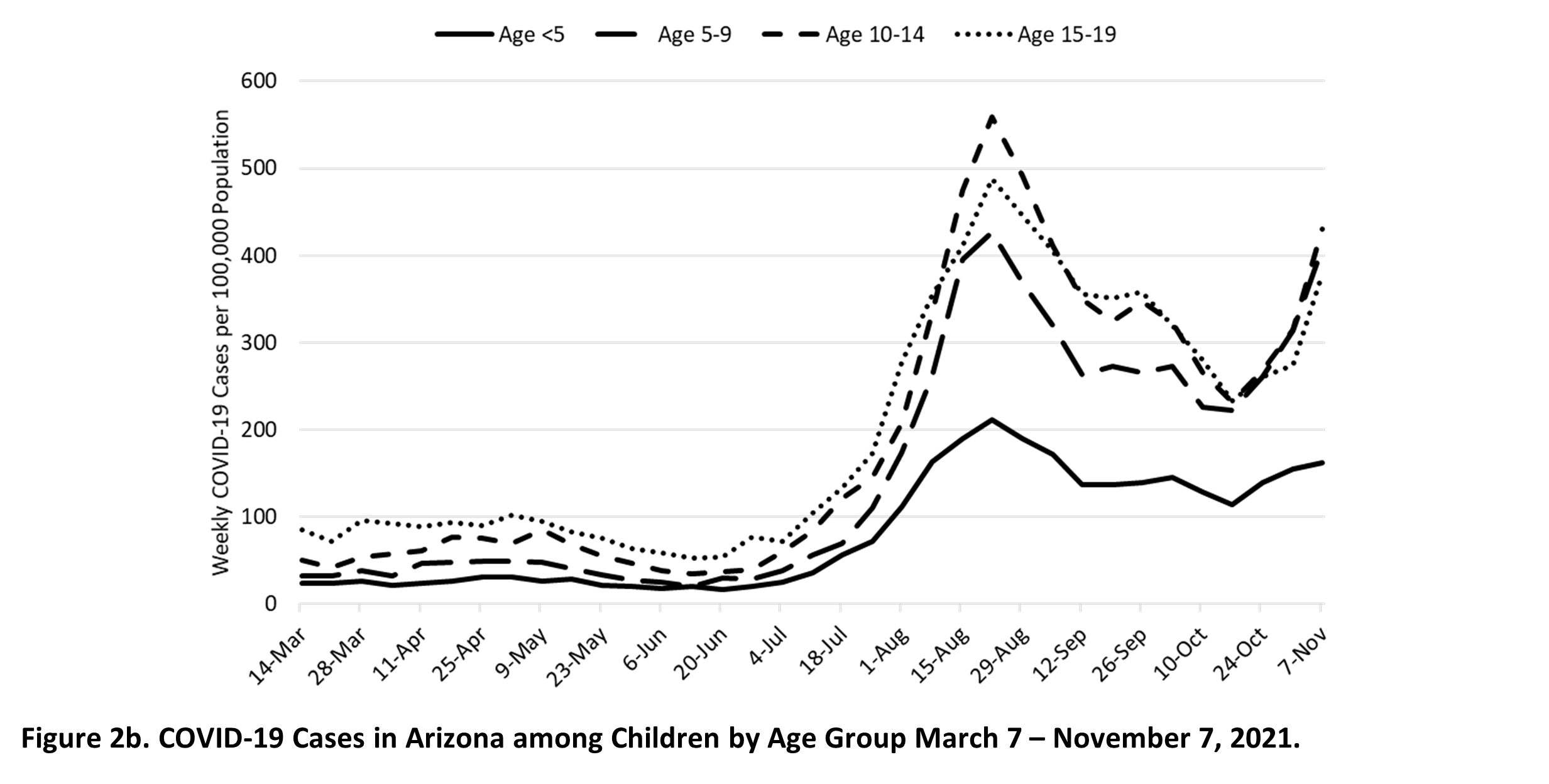
The death rate from COVID19 among kids was 250% higher in Arizona than the rest of the country (due to Governor Ducey and former Director Christ’s hostility toward evidence-based COVID19 mitigation measures). The direct COVID-19 mortality rate in Arizona was 0.73 deaths per 100,000 children while the national direct COVID-19 mortality rate was 0.27 per 100,000 children.
The most important parts of the report are the policy and operational recommendations that begin on Page 82 of the report.
We encourage every public health professional to review the recommendations before the legislative session and bookmark this report- as this is a must-have document for public health professionals committed to evidence-based policy.