Because Monkeypox virus is closely related to the virus that causes smallpox, the smallpox vaccine can protect people from getting monkeypox. Past data from Africa suggests that the newest smallpox/monkeypox vaccine (called JYNNEOSTM) is about 85% effective in preventing monkeypox (vaccination promptly after a monkeypox exposure may help prevent the disease or make symptoms less severe).
For many years, the U.S. has had a Strategic National Stockpile (SNS) of different kinds of therapeutics, vaccines and other materials that can be used in a public health emergency. Those stockpiles are stored in secret warehouses around the U.S. and can be drawn upon at the order of the HHS Secretary.
Smallpox was eradicated in 1979, but the smallpox vaccine has been included in the Strategic National Stockpile as a safeguard in case the smallpox virus is accidently or intentionally released from one of the two secure laboratories where it exists (at the CDC and the Russian Centre for Research on Virology and Biotechnology in Koltsovo, Russia).
So, if the smallpox vaccine works for monkeypox, and the smallpox vaccine is included in the SNS, how come the monkeypox vaccine is in such short supply? Note: Arizona has only received about 2,000 doses of JYNNEOSTM with 1500 doses on the way the way later this week.
The answer lies in what kind and how much of each of the smallpox vaccines are in the stockpile. The Strategic National Stockpile has three kinds of smallpox/monkeypox vaccines that are either approved or authorized for monkeypox:
- ACAM2000® – is approved for smallpox in persons over 1 year-old & is authorized under an Investigational New Drug protocol for monkeypox. It’s a “replication-competent live virus” (Vaccinia virus) which means that it’s a live attenuated virus that replicates. While the vaccine is fairly safe, it can cause myocarditis and/or pericarditis after administration (at an approximate rate of 5.7 per 1000). There’s also documentation that vaccinia can spread from person-to-person post-vaccination (ACAM can replicate). There are more than 100 million doses of ACAM2000® in the SNS.
- JYNNEOSTM – is the approved for both smallpox & monkeypox – but only for persons 18 years old and up. JYNNEOSTM is also a live virus but it’s not “replication-competent” which means that it can’t replicate like ACAM can. It isn’t associated with any cardiac adverse events like ACAM2000®. It’s also better tolerated and has fewer nonserious side effects. For that reason, in November 2021, the ACIP unanimously voted in favor of JYNNEOS as an alternative to ACAM2000 for primary vaccination and booster doses for both monkeypox and smallpox. There are only about 65,000 doses of JYNNEOSTM in the SNS – although HHS has ordered 2.5 million more doses from Bavarian Nordic A/S (a fairly small manufacturer).
- Aventis Pasteur Smallpox Vaccine (APSV) is also in the stockpile but this one is just an investigational vaccine that can only be used in a smallpox emergency under the right regulatory mechanism (Emergency Use Authorization). I can’t find how many doses the SNS has for this one.
Why Not Just Order ACAM2000 from the Stockpile to Increase the Supply Fast?
HHS will allow states to order ACAM2000® from the stockpile to increase their vaccine supply fast, but it appears that very few if any states are doing so. Why?
Like any other public health intervention, the first thing you need to do is look at the risks and benefits. ACAM2000® can cause serious reactions including myocarditis and/or pericarditis, encephalitis, encephalomyelitis, encephalopathy, progressive vaccinia, generalized vaccinia, severe skin infections, erythema, eczema, blindness, and fetal death in pregnant women.
For example, based on clinical trials, myocarditis or pericarditis (such as chest pain, raised troponin/cardiac enzymes, or ECG abnormalities) occur in 5.7 per 1000 primary vaccinations with ACAM2000. And remember, ACAM can replicate, so there’s a chance of vaccinia spreading from a vaccinated to an unvaccinated person.
Note: ACAM2000® isn’t approved for monkeypox, it’s just authorized for use with monkeypox under an IND protocol. By contrast, JYNNEOSTM is approved for monkeypox (but only for persons 18 years old and up).
JYNNEOSTM causes more typical and less problematic reactions like pain, swelling, inflammation, or itching at the injection site; muscle pain; headache; fatigue; nausea; fever; and chills.
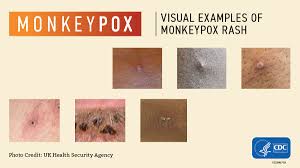
Now for the benefit side of the equation. Monkeypox can be a painful disease characterized by fever, headache, muscle aches, chills, exhaustion, and a painful rash that can look like pimples or blisters that appears on the face, inside the mouth, and on other parts of the body, like the hands, feet, chest, genitals, or anus.
The rash goes through different stages before healing completely. The illness typically lasts 2-4 weeks. Importantly, monkeypox is rarely lethal.
I’m not in charge of deciding whether to order ACAM2000® from the stockpile (that’s up to Mr. Herrington these days) – but if I were in my old ADHS director job, I’d stick with just ordering JYNNEOSTM even if it meant that I’d have less vaccine on-hand. The risks of using the vaccine outweigh the benefits from slowing the spread of monkeypox.
If there were an accidental or intentional release of smallpox virus (e.g., from the Russian Federation) it would make total sense to order and use ACAM2000® from the stockpile for a targeted ring vaccination campaign.
Why? Because smallpox variola major (the most common type of smallpox infection) has a mortality rate of approximately 30%… and the benefits of using the vaccine for targeted ring vaccination to respond to the smallpox outbreak/epidemic would greatly outweigh the risks of using ACAM2000®.
Pediatric Note: ACAM2000® is approved for smallpox for ages 1 year and up. However, it’s only authorized under an IND protocol for monkeypox. JYNNEOSTM is approved for monkeypox but only in persons 18+.
With pediatric cases and contacts now being reported in the U.S., an emerging pediatric care question is whether to administer JYNNEOSTM to pediatric patients off-label for post exposure prophylaxis or stick with ACAM2000® under the IND protocol. Seems to me the obvious choice is to administer JYNNEOSTM or forego post-exposure prophylaxis.
Historical Note: ACAM2000® was licensed by the FDA in September 2007. Prior to that, the smallpox vaccine was called Dryvax. If you think ACAM2000® has negative side effects and potential adverse events, wait until you read about Dryvax (Dryvax stockpiles in the U.S. have been destroyed).