|
|

|

|
|
|

Last week the Centers for Medicare & Medicaid Services approved AHCCCS’ request to begin reimbursing Community Health Workers for services provided to Medicaid members. CHWs are an integral and essential part of the health care delivery system, often at the front lines of the intersection between communities and health care providers.
CHWs often are also known by other names, such as Community Health Representatives, Patient Navigator, Promotores de Salud, Community Health Advisors, and Cultural Health Navigators, to name a few. Approval to reimburse CHWs for services is effective April 1, 2023.
Last week’s action brings full circle to the multi-year effort to build a reimbursement pathway for CHWs in Arizona. Way back in 2016 a group of stakeholders including AZPHA began pressing to give the ADHS the statutory responsibility to certify CHWs, a pre-requisite for reimbursement under Medicaid.
We succeeded in getting that authority in 2018 when the Arizona Legislature passed House Bill 2324, requiring ADHS to establish qualifications, a scope of practice, and core competencies for Certified Community Health Workers. That bill was successful due to the tenacious work be then Representative Heather Carter. See the ADHS Community Health Workers web page.
Starting April 1, 2023, AHCCCS and their contractors will be able to reimburse certified CHWs when their services are recommended by a physician or other licensed practitioner of the healing arts acting within the scope of authorized practice.
Services must be documented in the member’s medical record and may include health system navigation and resource coordination, health education and training, and health promotion and coaching.
AHCCCS has three billing codes for CHW’s: 98960- patient education & training for 1 patient for 30 minutes; 98961- for a group of two to four patients; and 98962- or a group of five to eight patients.
CHW Certification Portal Now Open
Arizona’s Community Health Workers can apply for voluntary certification once they show they meet the standards and have successfully completed an approved training program. Here is the ADHS certification portal. ADHS is using a federal grant to temporarily bring the certification fee down to $1, but that will end when the grant funding ends. Applications are fully electronic and available at azhealth.gov/CHW.
Report: Building Community Health Workers into the Continuum of Care
How to Get Your CHW Training Program Certified
The Tumblers Click: Community Health Workers Entering Arizona’s Care Network at Scale
AzPHA is a supporter of SB1710 which would change the governing structure for the Arizona State Hospital (ASH) from one in which the Arizona Department of Health Services both runs and ‘regulates’ ASH to a model in which the hospital operations would be managed by an independent governing body. The hospital Superintendent would report to the governing board rather than the ADHS Director. ADHS would then regulate the facility without an institutional conflict of interest.
The current governance structure for operating and regulating the Arizona State Hospital is fundamentally flawed because ADHS both runs and regulates the hospital. The lack of independent regulation and oversight results in poor accountability and can lead to unchecked substandard care when ADHS leadership soft-pedals regulatory oversight to give the appearance that the facilities are providing care that meets standards.
There is evidence that this occurred during the Ducey Administration. Even after multiple suicides and once homicide, ADHS‘ licensing division concluded that no operating deficiencies led to those deaths.
For context read this article by Amy Silverman: Patient deaths at Arizona State Hospital raise questions about staffing levels, lack of oversight and this piece by Mary Jo Pitzl at the Arizona Republic
March 23, 2023 Update: SB1710 passed the full Senate with a vote of 27-2 and has passed all assigned committees in the House. It awaits a final floor vote in the AZ House of Representatives following Committee of the Whole. If it isn’t amended on the House floor and passes it would go to Governor Hobbs’ desk for a signature w/o returning to the Senate.
If SB1710 is passed and signed, the responsibility for running the Civil and Forensic units of the Arizona State Hospital would transition to an independent board appointed by the governor beginning 1/1/25. The ASH Superintendent would report to the new Board. ASH would still be regulated by ADHS, but the institutional conflict of interest would be removed as ADHS would no longer be responsible for actually running the hospital.
ADHS leadership during the Ducey administration and even ADHS’ communications director during the Hobbs era has suggested that the Center for Medicare and Medicaid Services provides sufficient independent oversight of ASH, an oft-told and misleading statement. To clear things up, we prepared this review of how the Arizona State Hospital is ‘regulated’ under the current model. We close with a review of why SB1710 is so important.
There are 3 components to the Arizona State Hospital (ASH)… the Civil Hospital, Forensic Hospital, and the Arizona Community Protection and Treatment Center (ACPTC). The regulatory oversight differs for the 3 components that make up ASH.
The ASH Civil Hospital provides treatment and care for persons that are court ordered to the facility for psychiatric care. The Civil Hospital at ASH is run and regulated by the Arizona Department of Health Services (ADHS). ADHS’ Licensing Division is responsible for regulating the Civil Hospital which the ASH Superintendent is responsible for its operation.
State law allows healthcare institutions like ASH’ Civil Hospital to enjoy a Deemed Status license from the ADHS. That means that the Civil Hospital can hire an accrediting body to accredit the Civil Hospital. Once accredited, the Civil Hospital turns in the accrediting report to the ADHS Licensing division, and the ASH Civil Hospital receives a License from the ADHS – even though the ADHS doesn’t do an inspection of the facility before issuing the license.
The ADHS pays The Joint Commission (TJC) to accredit the Civil Hospital. ASH Civil started hiring TJC to do that work when I was Director. I think we paid TJC something like $10K for that service. Here’s a link to the deemed status licensing information about the Civil Hospital: Licensing Statement of Deficiencies. ADHS accepts the accreditation in lieu of an inspection and issues the state license to operate on that basis.
While the ADHS doesn’t do any annual inspections of the Civil Unit (because of its ‘Deemed Status’), the ADHS Licensing division can send out surveyors to investigate complaints about the care at the Civil Hospital when they receive them. If the complaint is substantiated, the ADHS Licensing Division can require corrective action and has some enforcement authority like issuing civil money penalties or placing the facility on a provisional license or even seeking revocation.
You can see that ADHS ‘complaint investigations’ seldom substantiate the complaints they receive and seldom find deficiencies (with a few exceptions). Here’s the recent compliance record: Licensing Services Facilities Report (azdhs.gov)
Because Medicare and Medicaid (AHCCCS in Arizona) pay for some of the services at the ASH Civil Hospital, CMS requires ASH’ Civil Hospital to be Certified to their certification standards. However, CMS doesn’t do their own certifications. They contract with the ADHS Licensing staff on the 4th floor of the ADHS building to conduct the certification inspections.
ADHS licensing staff go out and check at the ADHS ASH Civil Units to see if they’re adhering to CMS’ certification standards (which are a little different from the actual ADHS healthcare Institution regulations). ADHS Licensure then sends their report to CMS Region IX in San Francisco and the report is blocked, copied, and pasted and is sent back on CMS letterhead.
ADHS both runs and regulates the ASH Civil Hospital. ADHS leadership often suggest that there are checks and balances in the regulatory system to send the message that the monitoring of care is rigorous. The fact is that CMS Certification is not an independent review of care at the Civil Hospital because the work is conducted by ADHS Licensing staff.
While it’s true that The Joint Commission accreditation is separate from ADHS, the ADHS voluntarily pays TJC for the accreditation surveys and TJC views ADHS as a customer/client. TJC is not a regulatory body, and they have no enforcement authority. TJC Accreditation inspections that document deficiencies can sometimes jeopardize their contract with their customer, which has a chilling effect on documenting deficiencies.
The ASH’ Forensic Hospital provides care for patients that are determined by the courts to be “Guilty Except Insane” or “Not Guilty by Reason of Insanity”. The Forensic Hospital is also both run and ‘regulated’ by the ADHS Licensing Division.
State law allows healthcare institutions like ASH’ Forensic Hospital to enjoy a Deemed Status license from the ADHS. That means that the Forensic Hospital can also hire an accrediting body to accredit the Forensic Hospital. Once accredited, the Forensic Hospital turns in the accrediting report to the ADHS Licensing division and receives a License from the ADHS – even though the ADHS doesn’t do an actual inspection of the facility. The ADHS also pays The Joint Commission (TJC) to accredit the Forensic Hospital.
When the ADHS Licensing division receives complaints about care at the Forensic Hospital they can send out surveyors to investigate those complaints. If the complaint is substantiated, the ADHS Licensing Division can require corrective action and has some enforcement authority like issuing civil money penalties or placing the facility on a provisional license or even seeking revocation.
You can see that ADHS ‘complaint investigations’ seldom substantiate the complaints and seldom do they find deficiencies (with some exceptions). Here’s the recent compliance record: Licensing Services Facilities Report (azdhs.gov)
Because CMS doesn’t pay for services at the Forensic Hospital there’s no need for CMS Certification of ASH’ Forensic Hospital.
The Arizona Community Protection and Treatment Center (ACPTC) provides residential and care services for people that are civilly committed by the courts to the facility as a ‘Sexually Violent Person’. The ACPTC is licensed by the ADHS Licensure Division. They are not accredited by The Joint Commission nor are they accredited by CMS.
The current governance structure for operating and regulating the Arizona State Hospital is fundamentally flawed because the ADHS both runs and regulates the hospital. The lack of independent regulation and oversight results in poor accountability and can lead to unchecked substandard care when ADHS leadership soft-pedals regulatory oversight to give the appearance that the facilities are providing care that meets standards. There is evidence that this occurred during the Ducey Administration.
SB1710 is a needed reform of the governance structure that would move operational responsibility for operating ASH to an independent Governing Board. ADHS would continue to regulate the facilities but would be relieved of the conflict of interest that comes with running and regulating the same facility.
Sadly, Governor Ducey’s team killed the bill in House Rules last year… but we’re confident that this year’s commonsense intervention (SB1710) will also prevail in the House. In the meantime, we’ll continue our advocacy to get this bipartisan bill to Governor Hobbs for her signature.

Last week and this week are known as ‘crossover weeks’ when most committees don’t meet to clear everyone’s calendar for floor votes. Days were quite long last week with the House of Representatives spending 12 hours voting on bills one day last week.
The only committee that met last week was the Senate Committee on Director Nominations, a newly formed special committee to evaluate Governor Hobbs’ nominees to lead state agencies (see my op-ed on my opinion about that committee’s work: Senate committee doesn’t ‘vet’ nominees. It sabotages them
There were three nominations on the agenda—the Department of Transportation (ADOT), the Department of Administration (ADOA), and the Department of Environmental Quality (ADEQ)—but only the ADOT and ADOA nominees were considered, and only the ADOT nominee was recommended for a vote by the full Senate.
After the Senate Committee voted against former ADHS Director nominee Dr. Theresa Cullen and with the record from this week’s hearing, we can expect a challenging road ahead for all of Governor Hobbs’ nominees.
The ‘Third Read’ (floor vote) calendar in the House tomorrow is a mile long – looks like it could be another 12-hour day? Calendars || Bill Status Inquiry. Monday’s calendar in the Senate is a lot shorter right now but could get a lot bigger (although there are far more House bills than Senate bills owing to the fact there twice as many members of the House as the Senate.
Here’s our Bill Tracking Spreadsheet for this week
Now that the conference is over, I hope to have more time to do a more narrative analysis of bills in next week’s update.
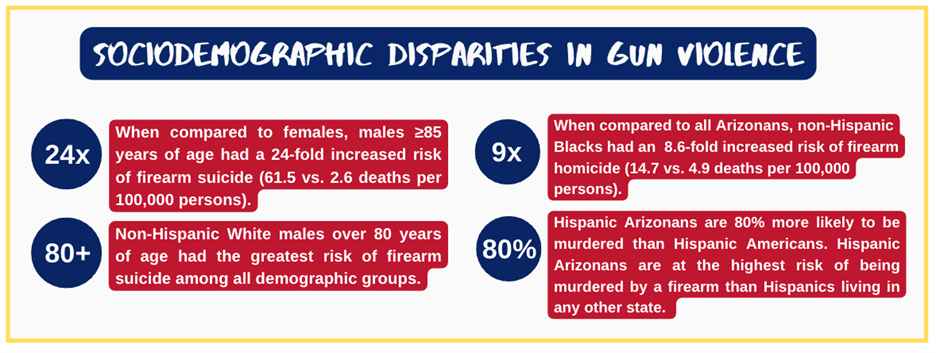
Last year the AZPHA Board of Directors got together for a strategic planning retreat. One of the outcomes was to develop strategic priorities for the next 2 years – which included prioritizing work around firearm violence.
The public health impact of firearm violence was clearly not a priority for state agencies including ADHS during the Ducey Administration, so we took it upon ourselves to fill that gap – much like we did by providing clarity during the pandemic.
All good public health work starts with surveillance and an evidence review… so we commissioned a report from Julia Jackman, B.S., B.A., an MSc Candidate in Global Health Fulbright Study & Research Grantee at the Norwegian University of Science & Technology to conduct the Arizona-specific surveillance and the literature evidence review.
Allan N. Williams, MPH, PhD Adjunct Assistant Professor, University of Minnesota School of Public Health Retired, Chronic Disease & Environmental Epidemiology, MN Dept. of Health served as her mentor throughout the months-long research project.
The report is finished, and we expect to publish our findings next week in a report entitled:
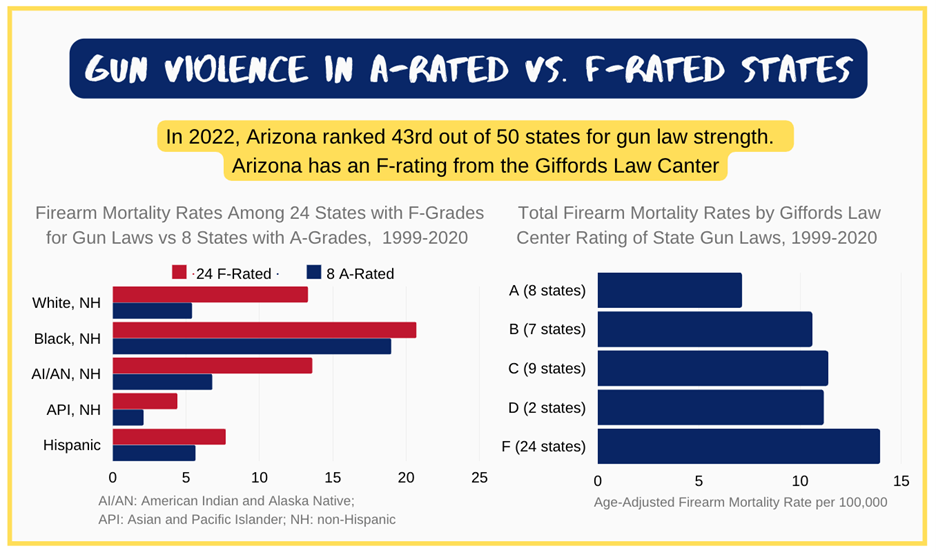
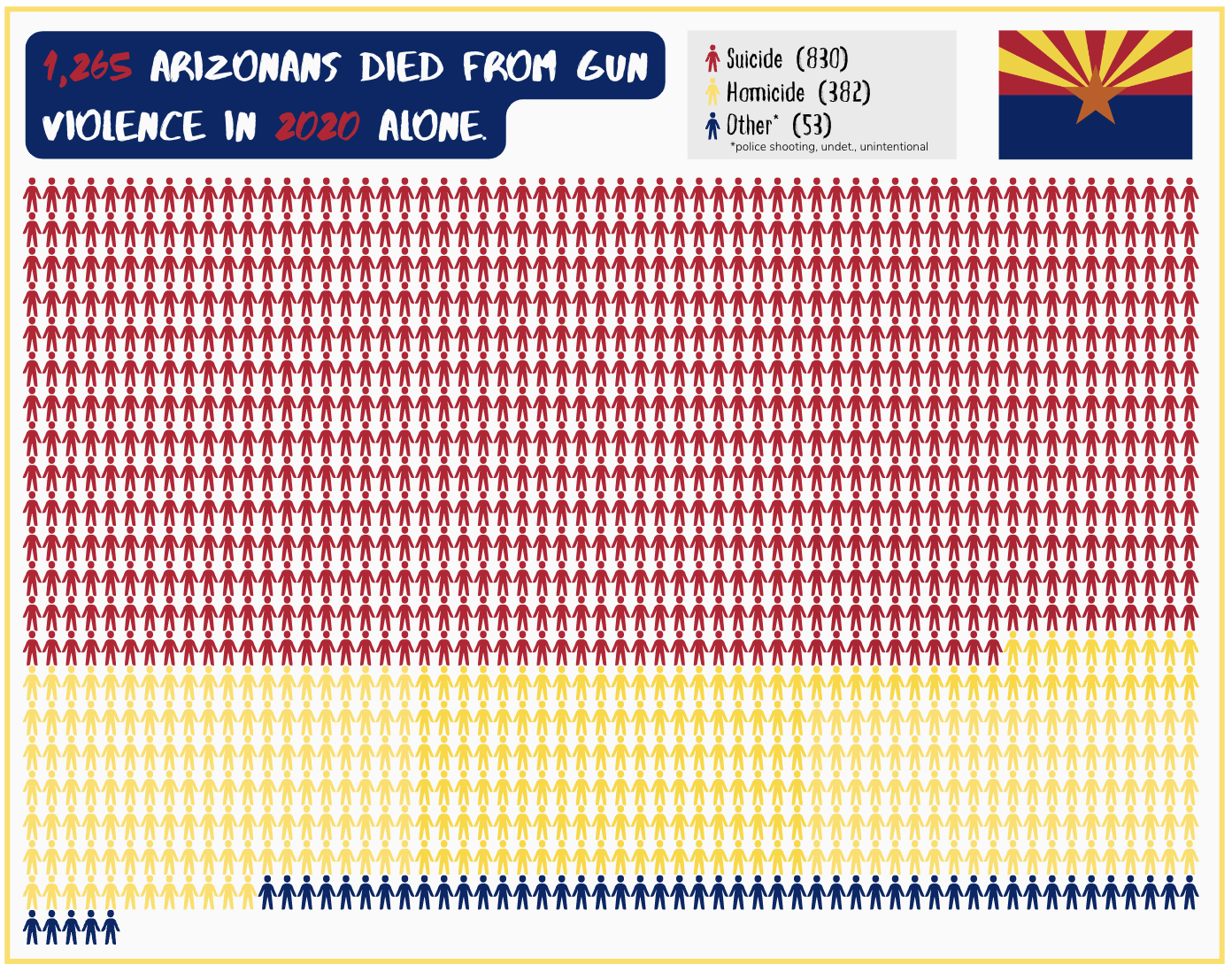
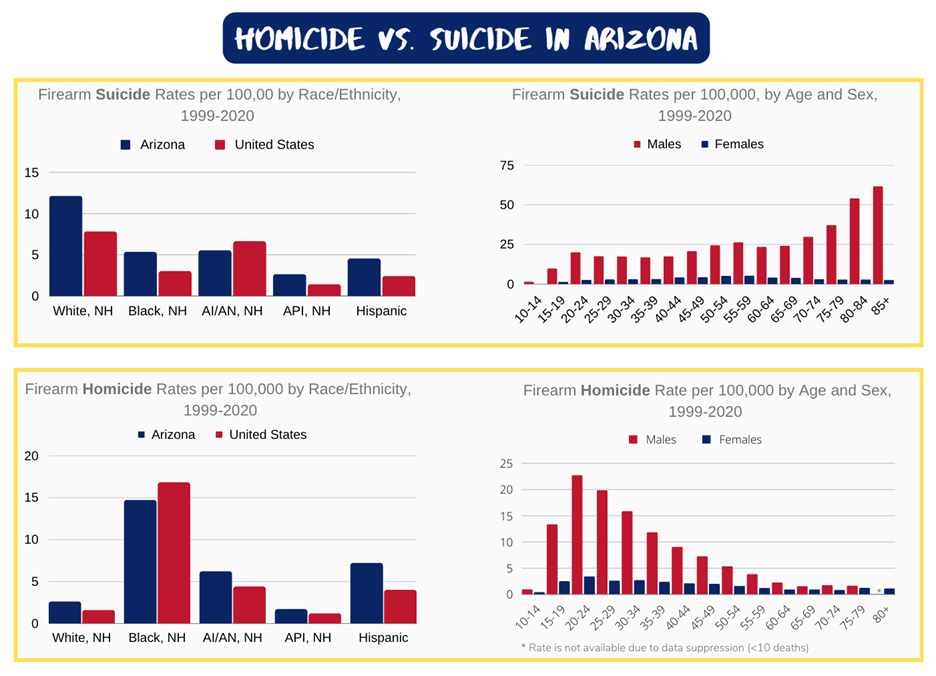
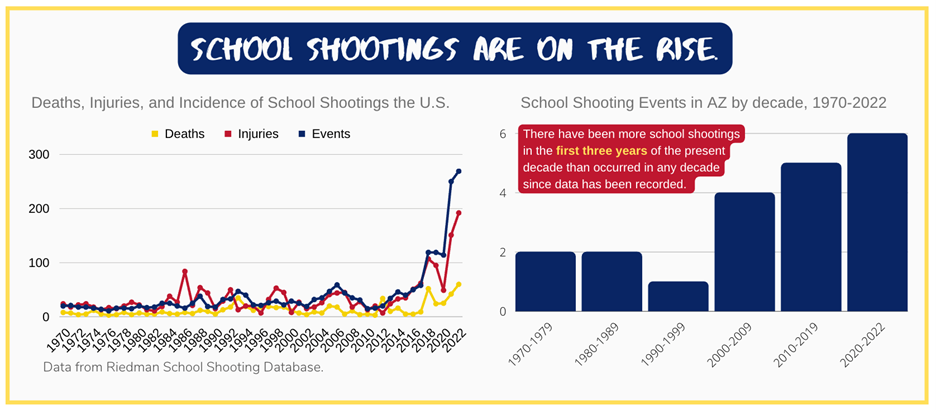
Gun Violence in Arizona Data to Inform Prevention Policies
The objectives of this report include:
Stay Tuned!