View Dr. Joe Gerald’s Weekly Epidemiological & Hospital Occupancy Report
The situation in Arizona hospitals is becoming increasingly dire. The number of available ward beds are now at the lowest point they have been during the pandemic. Access to care will continue to be restricted in the face of staff shortages in inpatient and outpatient settings. There’s undoubtedly primary and probably secondary triage happening already, and many Arizona hospitals are likely already operating under Contingency Standards of Care.
Read More About Contingency & Crisis Standards of Care
As of November 17th, 2403 (27%) of Arizona’s 8774 general ward beds were occupied by COVID-19 patients, a 14% increase from last week. Thirty-four percent (34%) of Arizona’s 1782 ICU beds are occupied by COVID-19 patients, a 12% increase from last week.
COVID-19 hospital occupancy is holding steady and will likely exceed 25% of all beds in the general ward and 30% of beds in the ICU for the remainder of the year. Because ADHS uses licensed beds in the denominator of their occupancy statistics rather than staffed beds- there’s less room at the inn than meets the eye.
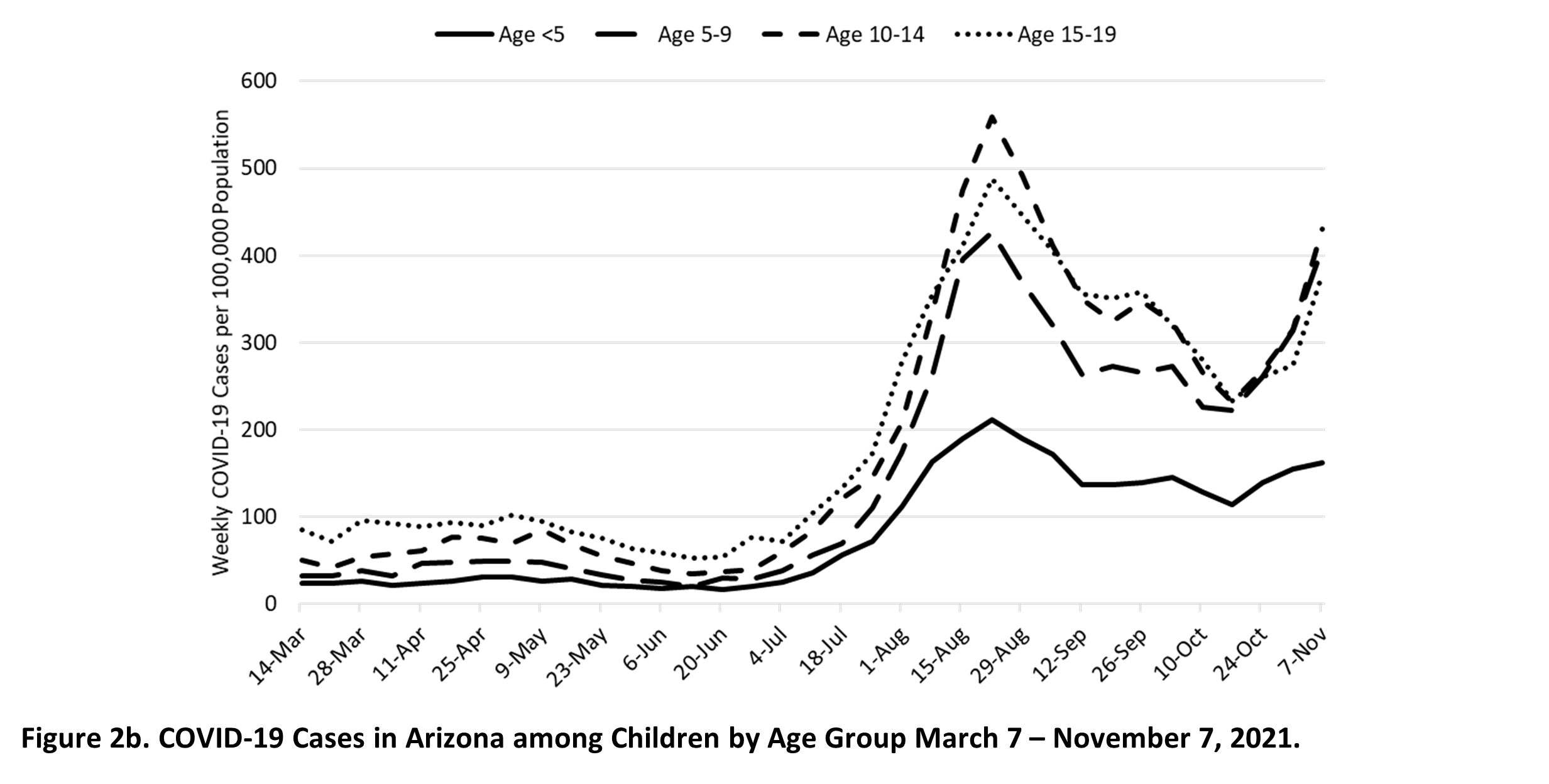
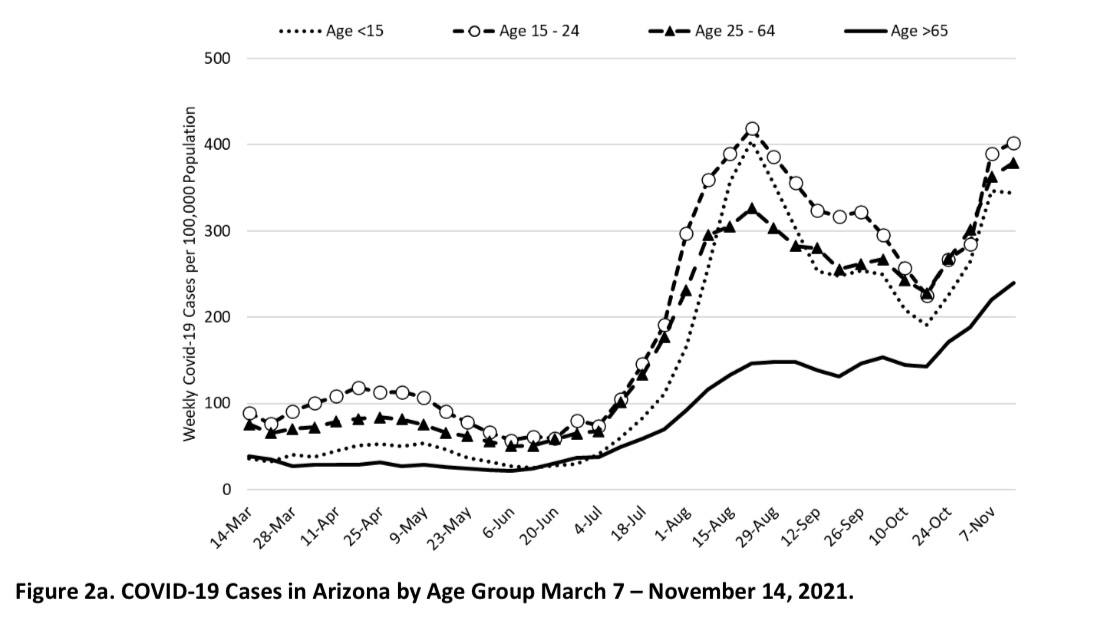
Arizona also continues to experience high levels of community transmission. Test positivity also remains high reminding us that test capacity, accessibility, and/or uptake is inadequate. Increasing case rates among older, highly vaccinated groups serves as a warning that major behavioral shifts and/or waning immunity could result in future increases in not only cases but also hospitalizations.
New cases were being diagnosed at a rate of 347 cases per 100K residents per week. The rate was increasing by 13 cases per 100K residents per week. Navajo, Greenlee, and Gila counties have case rates nearing their previous pandemic highs.
Meanwhile, Governor Ducey & Interim Director Herrington continue to nonchalantly shrug their collective shoulders.
View Dr. Joe Gerald’s Complete Weekly Epidemiological & Hospital Occupancy Report